Hopefully, this will answer most of your questions about using warm compresses, lid hygiene, and dry eye treatments. Please use your FIND bar to find your question/answer.
If you are a patient of mine and still have questions that were not answered below, please email Sheyda at smoreno@voeyedr.com
Thank you.
SLC
GENERAL DRY EYE QUESTIONS
Q. What are the general measures to determine if I have dry eyes?
The eye doctor or surgeon will look at all the layers of the eyeball to determine if a patient has dry eyes. The key components are as follows:
1. The Meibomian Glands: meibography (see below) allows us to now see how the oil gland layer is doing. We can see the glands disappearing if scar tissue is taking over.
2. The Goblet Cells: we cannot image the goblet cells, but any irregularity of the conjunctiva, such as Conjunctivochalasis (CCH), pterygium or pinguecula, traumas, or growths can disrupt the goblet cell layer. The only way to image the goblet cell layer is with Confocal Imaging and/or Impression Cytology: both of which are expensive, cumbersome, and currently used in research protocols.
3. The Lacrimal Gland: this gland produces the aqueous or watery part of the eye. It is hard to image the gland. MRI and CT provide little information in terms of the health of the ductules and composition of the aqueous.
Thus the way to determine if someone has dry is as follows:
1. Corneal exam: we look under the microscope at your eyeball's surface and lids.
a. SPK or Superficial Punctate Keratitis shows the patient has severe dry eye. This needs to be treated urgently.
b. Pannus: new blood vessels (ie, inflammation) is creeping onto the cornea usually due to a lack of oxygen supply to the cornea or local inflammation. This can lead to scar tissue and/or a corneal infection if not controlled.
c. Ulceration: a break in the cornea's epithelial layer can set a patient up for a corneal infection and loss of vision.
2. TBUT: Tear Break Up Time:
This determines the health of the meibomian gland layer or meibum to keep the tear lubricating the surface without evaporating too quickly.
3. Schimers' Test:
These are filter papers that measure the tear production in 5 minutes. This is usually performed with anesthesia (Schirmer I).
Q. What does a Low Schirmers' Test mean?
A low Schirmer’s test, though a nonspecific test, usually means the Lacrimal gland is not producing as much aqueous fluid compared to normal controls. The cause of a low Schirmers includes the following:
a. aging changes
b. genetic variation
c. autoimmune disease (ie, Sjogren's syndrome, Lupus, Rheumatoid Arthritis)
d. your body is not showing us the reason yet
e. Tumor infiltration: very rare.
As long as the blood work for autoimmune disease is normal, we do not usually do further work ups unless we feel a mass as the MRI or CT tells us little about the underlying pathology of the glands (ie, it will mainly tell us the size and if there is a tumor which is rare). Doing a lacrimal gland biopsy is reserved for end stage cases as the biopsy itself can lead to more scar tissue in the lacrimal gland, which we want to avoid.
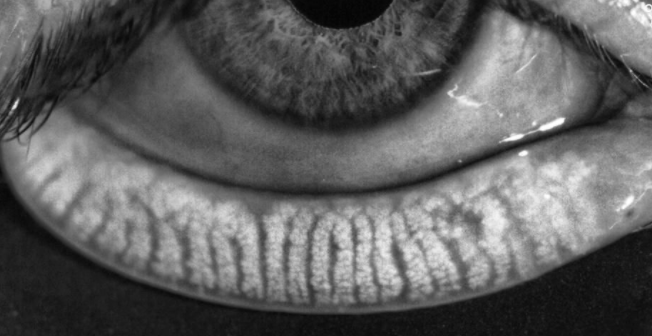
Q. How does Dr. Cremers see the meibomian glands?
Dr. Cremers: Before meibography was developed, surgeons and doctors could only see the outlines of the meibomian glands on the slit lamp, as seen below:

Now we can see the glands in more detail through meibography.
Q. I have been drinking decaf coffee ever since I was diagnosed with dry eye syndrome, but would like to return to regular coffee. Would regular coffee be fine for patients with dry eye syndrome?
Dr. Cremers: There should be no harm in some coffee, since there haven’t been any studies on its effects on dry eye.
Q. Is there a good/bad time to start trying to conceive if you are seeking dry eye treatment in the near future?
Dr. Cremers: No, there isn’t. However, you just cannot have stem cell injection done or be on steroids in the first trimester of pregnancy.
Q. I take oxybutynin at night: is this likely to be contributing to dry eyes?
Dr. Cremers: Yes, oxybutynin can cause dry eyes. Avoid using it if at all possible.
Q. I know you recommend PRN Omega 3 dry eye supplements or HydroEye for your patients. I was actually taking both of these prior to my first appointment with you. Is there a benefit to taking both, or are they redundant?
Dr. Cremers: There are no studies that say you need both. Some patients have said they feel a difference when they take 4000 mg medical grade Omega 3 vs 2000: but it is not a randomized controlled study. Each patient is different and responds differently to Omega 3 high dose vs. lower doses.
LID HYGIENE QUESTIONS
Q. Is there a limit as to how much I should do warm compresses?
Dr. Cremers: There is no limit, just do not burn your skin. There is no evidence that frequent warm/hot compresses damages meibomian glands. Some patients have sensitive skin so cannot do warm compresses often. When you feel grittiness, foreign body sensations, close your eyes and try to get a warm compress on them with lid massaging and hard blinking. This is trying to get the oil from the meibomian glands flowing If I feel the need to close my eyes, I’ll probably want to do something to get the oils flowing - whether that be lid massages/exercises or using a warm compress.
Q. I wear a silk sleep mask to bed. How often should I wash it?
Dr. Cremers: Likely every couple of weeks. No infection has ever been reported from a silk sleep mask. There has been one anecdotal report of a corneal infection in a patient who used press & seal over eye with gel in the eye: it is not clear if this
Q. I saw in your video that you used tree tea oil directly from the bottle. Is it o.k. to do that? You also mention to dilute it to 50%.
Dr. Cremers: It is. Put on a wet towel and I quickly tough the tea tree oil bottle top with it to semi-dilute it. Some patients need a wetter towel to dilute it more as needed to clean your closed eyelashes after the warm compress routine.
Q. What is your favorite Tea Tree Oil Brand?
There are so many brands. Here are some of the ones I love. The key issue is to dilute it before it hits the outside of your eyelashes or you will feel a bad burning sensation.
Cliradex wipes also work very well and are sort of "pre-diluted" though some patients have to dilute even more (dip edge or cut up piece in a drop of water).

Q. What other options are there to clean my eyes if my skin does not tolerate the diluted Tea Tree Oil?
Dr. Cremers:
a. Avenova is a prescription spray that does not burn that works well to clean off mites and bacteria. Ask for an Rx.
It is more expensive than Tea Tree Oil, but our office has coupons to help.
b. Hypochlorous Acid or Hypochlor works well for many patients as well. It is essentially diluted pool water but helps with killing mites.

Q. Can You Make Time to Observe My Lid-Cleaning Regimen?
**There is really no randomized controlled study on how best to do the warm compress routine, other than the research Dr. Korb has done:
http://eyedoc2020.blogspot.com/2017/02/how-best-to-clean-my-eyelids-controversy.html
Doctors recommend: do not burn your skin and do not hurt your eye applying pressure or massaging (ie, if you feel pain, stop what you are doing; if you skin peels, cut down on heat & timing). 10-15 minutes is idea. Other than that, I cannot say with authority which is the best way in terms of massaging the eyelid side to side versus up and down.
GENERAL DROPS QUESTIONS
Q. I am using Retaine and it feels like it doesn't adhere to the eye- they work well, but is there something I can try to make sure they settle in the eye?
Dr. Cremers: Close the eye after use then tape the lids afterwards.
Q. PRP drops Q & A Below:
Q. Why do my PRP bottles get clogged?STEROID DROPS QUESTIONS
Q. In the morning, I used Lotemax and felt a prickly pain sensation across both eyes like mini jabs of needles.The pain decreased then went away in 30-60 seconds. I’ve used Lotemax before without an issue. Is this of any concern?
Dr. Cremers: That can be normal. As long as you have no worsening pain or itching.
ADVANCED TREATMENT QUESTIONS
Q. What is IPL and are there risks?
Dr. Cremers: IPL stands for Intense Pulse Light. IPL has been used for more than a decade for the treatment for rosacea and acne. IPL uses Xenon flashlamp to emit wavelengths of light from 400 to 1200 nm. When placed on the light, a filter restricts the wavelength to the visible light range of ∼500 nm. When applied to the skin, this 500 nm light causes the blood cells in the abnormal telangiectasias to absorb the light, coagulate, and to constrict surrounding superficial blood vessels. Additionally, it appears to liquefy the abnormal viscous meibum and dilate the meibomian glands very well to help allow easier expression of viscous oil. Complications are rare after IPL for the eye. I have never seen depigmentation or even early stye formation after IPL in over 100 eyes treated with IPL as of 2018. The worst thing so far that I have seen with IPL is no significant in dry eye relief which happens in less than 5% of patients. The frustrating issue with IPL is that its effect may not last months or even weeks in some patients and sometimes more than 4-6 treatments are needed. Some of my patients come in every month for 1 treatment as that keeps the pain under control.
Also see: http://eyedoc2020.blogspot.com/2017/02/intense-pulse-light-ipl-risks-and.html
http://eyedoc2020.blogspot.com/2018/07/is-ipl-safe-does-ipl-work.html
More questions:
1. Who performs the IPL and probing procedures?
Dr. Cremers
2. What safety measures are used during IPL and/or probing procedures to guard the eyes?
Metal Contact Lens placed
3. Are there any anti-inflammatory protocols followed after IPL and/or probing to prevent
scarring?
Non-steroidal drops and/or steroid drops are used for 1-4days after the procedure depending on history of tolerance to medications.
4. Are maintenance procedures of Lipiflow/IPL/probing needed?
Usually yes; Lipiflow is recommended 2x/ year in patients who do not do warm compresses. IPL can be needed until oil comes out like "olive oil."
Probing: some patients need only 1 probing per eyelid to get full relief and others need multiple probing.
5. If needed, are serum tears an option in place of Xiidra/Restasis (especially for out of state
patients)?
Autologous serum 20% non-preservative can be used as a substitute or in conjunction with Xiidra, Restasis, Cequa.
6. With treatment, is it possible to predict prognosis at this stage?
Yes, depending on meibography of upper and lower lids, Schirmers test, Tear Break Up Time, and other risk factors mentioned below.
7. Are IPL useful even if the glands are not clogged ? Yes, IPL does help keep orifice open and keep oil gland pumping after expression after IPL. But it is usually expensive and uncomfortable so it is often reserved for patients with significant symptoms who also have poor oil (or little oil) coming out of glands.
8. The role of Lipiflow (ie, Thermalpulsation), IPL (Intense Pulse Light), MGP (Meibomian Gland Probing) in helping patients have less dry eye and neuropathic symptoms (ie, pain, reflex tearing, redness, itching, dryness, foreign body sensation, aching, discomfort, styes) and save meibomian gland structure and function can be very confusing. The reason is that there is no cure for dry eye and meibomian gland atrophy. The methods now available, which were not available a few years ago, try to slow down the process (ie Lipliflow), and IPL and probing try to help symptoms and restore meibomian gland structure and function. There have been few head to head comparisons among the three key options.
In general doctors and surgeons recommend treatments based on 2 key factors:
1. Age and Genetics (ie, family history of dry eye; Rosacea, Ocular Rosacea)
2. Meibography scores
(0= normal meibomian gland structure,
Grade 1=some loss of gland structure usually defined as less than one third of the total meibomian gland area, Grade 2=loss was between one third and two thirds
Grade 3=area loss was more than two thirds but less than complete loss
Grade 4=complete loss of glands.
3. Symptoms: How bad are your symptoms on a scale of 0-10 per eye?
4. Presence of risk factors: Autoimmune disease, previous Accutane use, previous Refractive surgery, deficiency of sex hormones notably androgens, Sjogren’s syndrome (SS), Stevens-Johnson Syndrome (SJS), psoriasis, atopy, polycystic ovary syndrome (PCOS) and hypertension, aniridia, chronic blepharitis, contact lens wear, eyelid tattooing, trachoma, Demodex folliculorum infection. Note: use of antibiotics, Isotretinoin for Acne, antihistamines, antidepressants, and hormone replacement therapy are found to be associated with MGD
5. Are you about to have eye surgery?
There factors may prompt a more agreessive approach to help prevent dry eye symptoms in the future which happens to many with aging.
In general, if symptoms are less than 3/10 with less than grade 3 meibography, I think Lipiflow is the best option as it is FDA approved and not painful.
If symptoms are above 3/10 we recommend a series of IPLs to get the symptoms below a 3/10. If worse than 6/10 in an eye, I usually recommend MGP/probing if IPL is not enough to keep symptoms below a 3/10 or if there is not enough good quality oil coming out of the meibomian glands (ie., oil is not coming out like amber olive oil but instead coming out as white toothpaste or not coming out at all).
IPL combined with MGP/probing appears to be the best option for fastest symptom relief if meibomian gland disease/atrophy is the key cause of symptoms and autologous serum, PRP, cord blood serum have been used or are being used to keep inflammation low.
XIIDRA Questions:
1. Xiidra is FDA approved as lifitegrast ophthalmic solution (Xiidra) to treat both the signs and symptoms of dry eye disease (DED) with an onset of action in as little as 2 weeks. But it usually takes 3 weeks of 2x/day use to feel an improvement. It's the first approved drug in a new class called lymphocyte function-associated antigen 1 (LFA-1) antagonists.
2. Can Xiidra be added to cyclosporine or in replacement? Yes it can. Some patients benefit from using Restasis and Xiidra together as they work on different inflammatory pathways. Most insurances, though, do not cover this.
Cyclosporine RESTASIS Questions: https://www.restasis.com/about-restasis-and-restasis-multidose
Q: How often can Restasis be used?
A: It is FDA approved for 2x per day. Some patients benefit from off-label used (ie not FDA approved) of 4x/day.
Q: I was on Cyclosporine in 2018. Then I stopped For 1 year and a half and I started again in July 2020 (so 2 months ago). Is it ok for the 3 weeks trial ( with the increased to 4 times a day ) because I heard the Cyclosporine takes at least 3 months to kick in?
A: Cyclosporine generally takes 3months to feel symptom relief as Restasis and 28d as Cequa; you can try use 4x per day which is not FDA approved but has been used by many patients to see if this helps. There are no known long term side effects of using this mediation. Thet most common side effects that go away after use are itching, burning, redness, tearing.
Q1. Are Scleral Lenses thought of as a short-term solution, long-term solution, or both? &
Q2: EyePrintPro scleral lenses. I am interested in trying them. What do you think about them?
A. Dr. Cremers: It can be both a short term and long-term solution.
I have many patients who use them for years. We do fit Jupiter here if needed.
A: Scleral Lenses have positives & negatives:
Positives: Scleral Lenses help some patients with discomfort by providing protection of the cornea from the wiper effect of the eyelid which can irritate corneal nerves. Some patients who have Corneal Neuropathy do not feel Scleral Lenses help symptoms. Patients who have "Lid Wiper Epitheliopathy" where the eyelid rubbing against the cornea causes pain, do report it helps and the use of Scleral Lenses can be both a short term
and long-term solution for these patients; but there are risks.
Negatives: The RISKS: all contact lenses are thought to affect the Goblet cells/Mucin layer through constant rubbing/trauma on these cells which compose an important part of the 3layered tear film (Meibomian Glands produce Oil, Lacrimal Gland produces Aqueous/water, Goblet Cells produce Mucin which help Oil & Water mix perfectly): though it is hard to image these delicate cells to prove this to patients.
Contact lenses and likely all scleral lenses have been reported to be a risk factor for Meibomian gland atrophy when used long term.
Each patient is different. In some cases, the benefits may outweigh the risks. As with many things, you might have to try them to see how our eye responds to them. If they are too irritating, you would have to stop them. If they help with redness, you could use them as sparingly as needed.
Though very rare, the key risk with any lens on the eye surface is a corneal infection which can lead to an eye infection and loss of vision. Thus if you use any contact lens or scleral lens, let your eyeMD know ASAP if you have any worsening pain, redness, or vision change.
The most commonly used Scleral Lenses are:
1. Prose (fit in Boston usually)
2. Jupiter (we fit these in our office but more recently our OD's like #3).
3. Synergeyes VS: https://synergeyes.com/
I am not familiar with the company EyePrintProb.
Q. My right is much worse and prone to redness/inflammation. Do you know why this might be, and are there any potential solutions?
A. If you are right handed, the theory is that people touch the right eye more than the left. If you sleep more on the right side, that could be an issue. Otherwise there is a 50% chance the right eye will be worse than the left.
Q. I have a small collection of blood vessels that have formed on my left eye right along my cornea. Is this permanent, or can it be removed?
This collection of blood vessels in the corner of the eye is usually called a pinguecula (or a pterygium if the growth crosses onto the Cornea -the window of the eye). Both can be removed with a surgical procedure that takes about 15min.
The risks of this surgery are rare but include: recurrence (the growth comes back; rarely more aggressively; infection (I have never seen this happen), the eye stays red (if new blood vessels are recruited to heal the defect (this is rare as well but is often due to local dryness: thus trying to treat the underlying dry eye issue is key as well). Sun exposure is the #1 cause of this growth. If you were rarely in the sun as a kid or now, let your eye surgeon know to send to pathology to be sure it is not a tumor (which is very rare as well).
Q. Do any of your patients have experience receiving partial or full insurance coverage for their cord blood serum drops? So far, no blood products are covered by insurance as it is a “natural product,” and not considered a drug thus far.
Q. If you are a patient with a mild bleeding disorder, are there any complications to Meibomian Gland Injection/Lacrimal Gland Injection?
Dr. Cremers: So far there are none, even in patients on Coumadin. If we have to do anesthesia with a needle (which is rare) for pain relief, there will be bruising/black and blue bruising around the eyelids which can last days to weeks depending on the blood disorder or blood thinner one is taking.
Q. Can you take fish oil before the Meibomian Gland Injection/Lacrimal Gland Injection?
Dr. Cremers: Yes, you can.
Q. Are any contraindications to pregnancy planning with PRP injections?
Dr. Cremers: No, there are none.
Q. I have scheduled an IPL (Intense Pulsed Light) on my next visit with PRP injection. I was wondering if perhaps a Lipiflow might be helpful on one eye in the meantime, and if so, when should I get it?
Dr. Cremers: Lipiflow is a good idea to keep oil pumping, but if you are getting IPL, this should do the trick as well. I do not think there is any harm in doing Lipiflow 2x per year, as recommended by the manufacturer, but has not been studied beyond that in terms of its effectiveness. If done, I would recommend you do it in about 2 weeks.
Q. Should I be applying mineral oil to my eyelids (per the post-Lipiflow instructions) at this point?
Dr. Cremers: Yes you can; however, some patients prefer coconut oil.
Q. I’ve been having some light sensitivity—is that likely from the Lipiflow or the Lotemax?
Dr. Cremers: Dry eye is the number one cause of light sensitivity. If it does not improve, let me know.
POST-MEIBOMIAN GLAND PROBING AND PRP INJECTION QUESTIONS
Q. What is Meibomian Gland Probing?
Meibomian Gland Probing with Expression (MGPE) (eg: often referred to as "probing," it is important to be sure your surgeon is also expressing as many meibomian glands as possible) is a minor procedure where the surgeon takes a sterile probe or cannula (ie, it is not a needle) and enters the meibomian gland with the goal of breaking open scar tissue within the gland and/or at the orifice. MGP should always be performed with oil expression where a sterile apparatus or cuetips are used to milk the oil out of the glands after the scar tissue is opened. The idea is that by relieving the blockade within the glands, the oil can come out which will lead the body to produce more meibomian gland oil. An analogy, though imperfect, is like having a blocked breast milk gland for a nursing mother: these can be very painful until the blockage is resolved. Meibomian Gland Probing with Expression can be performed with or without insertion of Autologous Serum, Platelet Rich Plasma, or Autologous (your own) Stem Cells.
MGPE can be uncomfortable and even painful. They do help relieve pain in the majority of patients, but they are not FDA approved. There have been a series of studies showing Meibomian Gland Probing and Expression help with eye pain from dry eye and revive meibomian glands, but the improvement is not 100% nor does it occur for 100% of patients. We have found some patients to have significant relief after one round (all 4 lids probed and expressed) but have required it to be repeated after a few months or even a few weeks. When we inserted a patient's own PRP into the glands the pain relief lasted longer. In 2 patients the insertion of autologous, adiopose derived stem cells provided approximately 4-6months of relief without needing a repeat probing during that time.
Patients with autoimmune induced meibomian gland dysfunction tend to need probing multiple times per year. This is an out of pocket procedure and not covered by insurance, unfortunately. Dr. Maskin in Tampa charges approximately $10,000 for probing of all 4 lids. We charge a fraction of this but the procedure is still expensive. Email Sheyda for more information: smoreno@voeyedr.com
Q. How is Meibomian Gland Probing Done?
We do this procedure under the microscope with sterile 1mm, 2mm, and 4mm cannulas. We start off using the 1mm cannula and move up in size if needed or if the patient did not find relief with the shorter cannulas. The 4mm probe is more uncomfortable so we use this probe if the shorter cannulas did not relief pain.
During the procedure, the patient's meibography images are available for the surgeon to determine which glands are fully scarred and which are not.
When using PRP: I usually insert PRP into all glands with the microscopic cannula as we have not seen anyone worsen from PRP inserted into viable meibomian glands. Still, I can make every effort to probe/or insert PRP into only the glands that do not look like they are producing oil (ie, meibum), if requested: I can make every effort to only inject the glands that are viable. Often fully scarred glands cannot have any probing or insertion of PRP as the orifice if completely scarred. Since the glands are very close together it can be hard to be 100% sure which glands are scarred inside the gland (ie, no visible scarring seen at orifice with microscope) and which ones are not.
Q. How Often Do I Need Probing?
Our usual schedule is probing again in 1-3 months depending on the amount of scarring and symptoms. We have patients who come in every month for probing and others who come in every 3months and still others who come in once a year for maintenance.
Q. I just had meibomian gland probing with PRP injection and I think my eye is infected. It is producing some goop and crust. Is this normal?
Dr. Cremers: This is normal. The probing releases inflammatory factors in many cases, which can make the eye feel more goopy and have crusting. I would advise you to follow the instructions below:
1. Cold ice packs for first 6 hours after probing to keep swelling and increased irritation to a minimum. Start warm compresses over lid margin area after swelling has decreased or if you notice minimal swelling.
2. It is ok to use over-the-counter Ibuprofen if needed (up to 600 mg three times a day) if needed.
3. Neo-Poly-Dex ointment twice a day inside the eyelid after the procedure for 1 week.
4. Non-steroidal anti-inflammatory drop: Prolensa or Illevro once a day or Ketorolac twice a day for 1 week.
5. Steroid Drops: Lotemax (weakest steroid drop), Predforte, Durezol (strongest steroid drop) 2-4 times per day for any increased irritation for 3-5 days after the procedure as needed.
The goal is to not to notice any increased irritation from increased inflammatory factors released during probing and to prevent inflammation which can close the meibomian gland orifice. But we also want to minimize total steroid use as much as possible.
Each person will need differing amounts of anti-inflammatory drops/pills depending on many factors such as:
General health, autoimmune risk status, diet (low inflammatory diet is best
How much Omega 3 intake per day (recommend 2000-4000 mg/day)
How often doing warm/hot compresses and using diluted tea tree oil/Avenova (if skin can tolerate recommend compresses and diluted tea tree oil/Avenova 2-3x/day)
Use of Doxycycline (recommend 20 mg/day if no allergy, not pregnant/nursing, won’t be in sun)
Genetics, age, and smoking/meds (i.e. Accutane) history.
Q. If there is pain afterwards, should I keep my eyes closed as much as possible to subside the pain? And if so, for how long?
Dr. Cremers: Some patients have pain after probing. Some patient have no pain.
If you do have pain, keep your eyes closed as much as you can and rest your eyes.
You can put cold compresses and take acetaminophen 500mg 3-4 times per day or ibuprofen 600mg 3-4 times per day if you have no contraindications.
It is not uncommon to have pain after any eye procedure. The pain that can occur after probing is thought to be due to the inflammatory factors released after probing and the microtrauma of the probe entering the gland orifice. Corneal abrasions have been reported after probing but are rare.
Q. When can I start wearing my contact lenses after Meibomian Gland Probing?
Long term contact lenses use increases the risk of inflammation which can damage the delicate cells of the conjunctiva (ie, the goblet cells that produce mucin) and meibomian gland cells. Still some patients feel they cannot live without their contact lenses.
We recommend you wait at least 24hrs before using contact lenses after probing.
But try to use your contact lenses for only "contact lens" worthy events.
Try to use your glasses as much as possible, especially on the weekends or when you do not need your contact lenses.
Q. What have been the results of PRP insertion into the Meibomian glands so far? Why do patients feel relief? Is it a cure?
Dr. Cremers: As of 2018, We are preparing a publication about our results so the final analysis is still pending, but we believe PRP is helping improve Meibomian gland function by stimulating the meibum cell to produce more meibum (ie, meibomian gland oil). We have seen gland improvement or “growing back” in 3 patients out of 11 thus far.
In our patients with autoimmune disease, where the immune system may be actively trying to destroy Meibomian glands, the glands can begin to atrophy again in future. Meibomian glands decrease in function with age: thus we do not have a proven cure yet for Meibomian gland dysfunction though most patients report an improvement after this procedure. One of the 11 patients did not improve after PRP was injected into a lacrimal gland: we believe this patient has neuropathy and the PRP did not help relieve symptoms.
Even though we have not had any complications with this procedure, PRP drops and insertion of PRP into meibomian glands is experimental and is not FDA approved. We perform this procedure on patients who have tried all FDA approved options and have not found relief from their eye pain or neuropathy.
Q. Is the needle for PRP injections the same size as the probe or bigger or smaller?
Technically, Dr. Cremers does not inject PRP into any part of the body with this procedure. The PRP is being inserted into the Meibomian Glands' orifice with a cannula. There is no needle used.
Some patients request lidocaine anesthesia injection around the area being probed as probing can be painful.
If lidocaine anesthesia injection is needed to help with pain, which is needed in a minority of patients, a 30G needle is used.
For the insertion of PRP into a Meibomian gland, the cannula is the same diameter and size as the usual meibomian gland probe.
Q. What’s the risks of steroid injections into the glands?
We do not inject steroids into glands but have inserted steroid with a cannula into the meibomian glands in the past.
We found that inserting PRP appears to be better tolerated with less risk. So far there
have been no complications or risks of inserting steroid into the Meibomian glands globally.
The risks of injecting a steroid into the skin is well known which includes a slight whitening of surrounding skin that can be permanent. The risk of embolism leading to loss of vision or even a stroke is very rare but has been reported.
Q. Should I resume squeezing eyes shut (hard blinking) due to the possibility of the PRP coming out of my glands? If so, when I should resume?
Dr. Cremers: Applying cold ice packs to the eyelids (eg, not too cold/not cold enough to hurt the eyelids) will help decrease inflammation and is recommended for the first 2 hours. After this warm compresses are restarted and hard blinking can resume.
Q. Is involuntary clenching (blinking while eyes are closed) okay after the procedure?
Dr. Cremers: That is ok to do.
Q. Should I return to using warm compresses three times a day as normal the following day?
Dr. Cremers: Keep cold ice packs on your eyes as much as possible without causing pain to the skin for the next 2-3 hours if you notice swelling. Start warm compresses tonight if there is no significant swelling (i.e. eyelids are swollen shut: which is very rare).
Q. How often should I do cold compresses?
Dr. Cremers: Cold helps decrease itching, swelling, and inflammation. Heat helps with cleaning, killing bacteria/mites, and naturally opening the orifice of meibomian glands. For swelling and itching, use cold compresses/ice packs as needed. Continue Warm compresses at least morning and night without burning skin or making swelling worse.
Q. Should I start using Avenova twice a day?
Dr. Cremers: Start using Avenova once a day to twice a day the night after the procedure.
Q. How do you know a gland is scarred?
Dr. Cremers: Meibography is an excellent way to determine if a gland is completely scarred. While meibography is not perfect for determining the level of scarring in gland (eg., the gold standard is taking a slice of the gland, putting it on a slide, and looking under a high powered microscope), it is the best we have for in-vivo (eg., in a live patient) viewing of glands.
Q. How can you tell a "normal gland" has no scar tissue?
Dr. Cremers: we look at the meibography and under the slit lamp microscope at each gland to see if the gland has any signs of scar tissue. The only way to be 100% sure there is no scar tissue would be to take a slice of the gland as noted above which is not done for clear reasons. The next best way is to use a probe to enter each gland. If there is scar tissue in the orifice, we can hear a pop or feel it pop open. We can also see scar tissue in the orifice of a meibomian gland under the microscope. Sometimes we cannot enter a gland with a probe because it is fully scarred.
Q. What does it mean when the "gland pop." Does that mean that scar tissue went away after being probed? Or is it still there/ always be there? Or will it come back?
A. The pop that the surgeon feels and/or hears (sometimes the patient hears the pop as well), represents scar tissue present at the orifice of the meibomian gland or within the gland that is broken through.
There are no publications to date to report that probing increases scar tissue formation in the meibomian gland. There is an internal battle between Dr. Toyos and Dr. Maskin on this subject: both have vested interests in IPL and probing, respectively. Dr. Toyos has noted that probing can potentially increase scar tissue, but there are no reports to my knowledge of this yet. Dr. Maskin has noted that one might damage the meibomian glands if you do IPL and express against a scarred orifice: there are no reports to my knowledge of this yet, either.
There are publications that show breaking open scar tissue can help oil released from the meibomian glands which can preserve, and in some cases restore meibomian gland function. My own research has shown this to be the case as well. Using a patient's own Platelet Rich Plasma (PRP) also seems to help restore gland function better and for longer than just probing in some patients. PRP insertion into the meibomian gland, however, is still in the investigation phase and has not proven with randomized controlled studies yet. Still, I am hopeful probing combined with Autologous Serum, PRP, autologous stem cell, and/or cord blood serum will hold the secret on how to regrow meibomian glands.
Q. How bad was the scarring of the ones that went pop? Partially scared or how bad? And how many glands were scarred that were probed? Will those scarred glands always have issues with the oil producing because they had some scarring do you know?
We usually count the pops which we believe represents scarred glands. The meibography is the best way to determine how many glands have scar tissue. There is no available “scope” to look inside the glands as of yet. Depending on the extent of the scar, many partially scarred glands can recover and produce normal oil again. I have seen this occur multiple times. A gland that is completely scarred with a scarred orifice is almost impossible to restore. My theory is that at least 1 meibum cell is needed to restore the function of the gland again. Some patients have a lid full of 100% scarred glands. I have not seen a report of being able to restore these glands fully. Thus we want to treat patients before the meibomian glands are replaced by scar tissue.
Q. Some of my glands were not probed and looked full on meibography. Could they have scar tissue? How can you be sure?
A. Some patients prefer not to probe all glands. Meibography is the best way we currently have of determining the presence of scar tissue in a meibomian gland. Meibography is not 100% accurate in all cases. The only way we could be 100% sure there is no scar within a gland is to cut the gland out, put it on a slide and look under an intense microscope: that would create more scar tissue and is thus not done. Also, we do not have “meibomian gland scopes” to look inside the gland with a micro-camera. Until these are available, meibography and slit lamp microscope viewing is the best we have and it is very hard to say for sure there is no scarring of an otherwise “normal appearing gland.”
Q. Why would there be scar tissue in a normal appearing gland?
The pathophysiology of meibomian gland scarring is currently being investigated to see why and how scar tissue forms. There are 3 key components/ theories. The truth of the cause likely is related to a combination of all 3.
The 1st is that scar tissue develops when the Orifice of the Meibomian Gland gets covered or clogged by scar tissue (ie, Rosacea patients, aging, genetics), bacteria, mites (ie, Demodex), make up, trauma. Once the orifice is blocked, the oil can not come out and the gland begins to down-regulate and begins to produce less oil. This sends a signal to meibum cells to stop producing meibum which can then become dormant and form scar tissue.
The 2nd theory is that some internal factors or risks (ie, autoimmune disease, such as Sjogren's Syndrome, Lupus, Thyroid issues, Rheumatoid Arthritis, and maybe even Rosacea) or toxic-to meibomian gland-chemicals or treatments (ie, Accutane Chemo, Radiation, trauma, lid surgery) can directly and internally destroy the function of the glands.
The 3rd theory is that increased surface inflammation (ie from many of the conditions discussed above including, autoimmune diseases, Rosacea, prior Accutane use, allergies, history of allergic conjunctivitis, Contact Lens Use, Previous LASIK/PRK, pterygium or pinguecula present, chemicals exposure can lead to scarring internally and at the orifice due to a higher amount of inflammatory factors around and entering in the gland.
Aging and genetics is a big component of general inflammation and scarring in the meibomian glands and elsewhere. There is a role of diet in the inflammation cascade as well but has not been fully described yet.
Q. If there is scarring in glands, does it mean the oil will always be thick and the gland scarred? Or can scarred glands produce normal oil again?
I have seen scarred glands begin to produce normal oil (olive oil color and consistency) after multiple probing and expression and/or multiple IPLs with expression. The usual progression of oil production is as follows: I call it--
The 7 stages of Meibomian Gland Oil Production: (see below)
One eyelid can have glands of different stages. Most patients find relieve when they are at stage 5 in the majority of their meibomian glands.
Oil can be classified in terms of Quantity (ie, amount of Oil expressed) and Quality (ie, the color and consistency).
Quantity: amount
0: none
1: very little nubbins of oil visible, even with forcibly milking and expression
2: more oil seen in as short strands
3: long strands of toothpaste oil
4: thick clumps of oil.
5: liquid "olive oil" like drops come out with expression
6: gush of "olive oil" comes out of orifice when pushed on gently
Quality: color and consistency
0: no oil visible
1: little white nubbins of oil seen even with forcibly milking and expression
2: more oil seen in as white "toothpaste" strands
3: long strands of white toothpaste oil: less thin, getting a little thicker
4: thick clumps of yellow oil or globs of oil come out.
5: liquid yellow "olive oil" like drops come out with expression
6: gush of yellow "olive oil" comes out of orifice when pushed on gently.
Putting it All Togther:
The 7 stages of Meibomian Gland Oil Production:
0: No oil visible. No oil comes out of the gland orifice: Sometimes no oil is expressed but with probing and/or IPL and expression, the glands begin to get stimulated and future treatments will lead to some oil production.
1: Little oil visible: little white nubbins of meibum oil seen, even with forcibly milking and expression
2. Short, Thin, White Strands: Meibum oil over time with multiple expressions can then begin to come out like “thin white strands of toothpaste” or “thin white ribbon.”
3. Long, Thin, White Strands: Then the oil with time with come out as longer thin white strands of toothpaste.
4. Thick Yellow Clumps: Then the oil will start to turn yellow and become thick strands of yellow toothpaste or ribbon.
5. Yellow Oil, not clumping or toothpaste: Then the oil will start to come out as yellow olive oil without clumps or strands.
6. Gush or flush of yellow olive oil: Then the oil will start to come out as normal “yellow olive oil” like fluid, even gushing out with expression. This is what it looks like in young normal patients without scarring, Meibomian gland disease, or dry eye symptoms.
While I have seen what looked like a completely scarred meibomian gland produce normal oil, it could be there was still one meibum cell still present in the gland that allowed the gland to re-form. Maybe the gland was not totally scarred. We are still not sure if the meibomian glands are like breast milk glands which have the ability to resume function if the right circumstances are in place (eg., for breast milk glands, the hormone Oxytocin is back after a baby is born).
Q. Do the scarred ones eventually atrophy?
Many patients over time develop scarred glands. Age, genetics, electronic screen time, medications, autoimmune status are risk factors.
Scarred glands that are not treated with Lipiflow, IPL, probing usually atrophy over time.
Blinking frequently and applying warm/hot compresses without burning the skin are key to avoiding gland atrophy.
Q. How bad would you say my rosacea? How can you tell? Could rosacea be blocking up my glands?
Rosacea blocks glands can destroy them over time due to chronic inflammation over years. Your rosacea is mild but present. Other environmental factors (such as a history of genetics, aging, history of chronic allergy, average time spent on electronic screens, contact lens use, Accutane, Autoimmune disease (thyroid issues, Lupus, Sjogrens Syndrome, Rheumatoid Arthritis, Ulcerative Colitis, etc), diabetes, chemo, radiation, trauma, refractive surgery) can increase meibomian gland atrophy risk even in patients who have mild rosacea.
Q. Do you think the eyelash tint would be making my dry eye worse/ causing it?
A. I do not think the eyelash tint is making it worse as it is not covering the orifice.
AUTOLOGOUS SERUM Questions and Answers
AUTOLOGOUS (means it comes from the patient) SERUM (the liquid or clear part of a patient's blood that is separated from the red blood cells or cellular part) has been used for years to treat a wide variety of eye surface disorders, such as severe dry eye corneal infections and ulcers, and other ocular surface disorders, such as Sjögren's syndrome (SS), superior limbic keratoconjunctivitis, graft-versus-host disease, Stevens-Johnson syndrome, ocular cicatricial pemphigoid, recurrent corneal erosions, neurotrophic keratopathy, Mooren's ulcer, aniridic keratopathy, and postkeratorefractive surgery.
I have prescribed AS for almost 18 years to help a patient's eye heal faster from inflammation, infection, autoimmune diseases, or other disorders.
AS has been proven to maintain the shape and function of the corneal cells much better
than pharmaceutical tear substitutes, since its biological properties are similar
to natural tears. AS contains a complex composition of water, salts, proteins,
vitamins, lipids, immunoglobulines and growth factors which are similar or even better in some cases than the biological nutrients that are found in a "good" or normal tears [1, 4–6]. Serum and tears show similar constituent concentrations, with the exception of greater amounts of vitamin A, lysozyme, transforming growth factor-β (TGF-β), and fibronectin and reduced amounts of immunoglobulin A (IgA), epithelial growth factor (EGF), and vitamin C in serum when compared with tears [1, 2, 4].
AS eye drops are prepared as non-preserved diluted blood solutions [1, 7–9] for most of these treatments. Sometimes 100% serum is used.
Even though many doctors and scientists worldwide have conducted studies that
show the benefits of using autologous serum drops, the US does not currently
have a Food and Drug Administration (FDA)-approved protocol or guidance for
this process since it is a patient's own blood and not a drug.
To make your eyedrops we will need to collect some of your blood in several
tubes and it will need to be allowed to clot for one to two hours. Then it will
be placed into a machine that spins the blood at a very high speed, causing
the red cells to separate from the serum. The serum will be taken and mixed
with non-preserved artificial tears or balanced saline solution at a specific concentration.
The bottles need to be kept in your freezer at home and you can remove one bottle at the time, leaving it to thaw in the refrigerator. This refrigerated bottle usually lasts 7-10days and is then thrown out.
Remember, after thawing, the bottle should be kept in the refrigerator at all times. Bottles cannot be left on the counter as bacteria can grow and lead to an infection (which Dr. Cremers has never seen but has been reported).
Most patients start out using AS 4x per day. Some patients feel relief with just 2x per day; some patients need to use them every hour.
AS eye drops improve the quality of life of severe dry eye patients, although reports of the correlation between this improvement and clinical measurements are scarce in the literature. There is no standard dilution of serum for use in anterior segment applications as each patient may respond differently to different dilutions. We usually start at 20% dilution, unless I feel a stronger % is needed or a bad corneal infectin is present. The more diluted the AS, the longer it will last. Some patients need 50% dilution. Some need 100% to feel relief. Time will tell what is the most diluted % of AS the patient can use and still feel relief.
Rarely, AS provides no relief. It used to be I could count on 1 hand the number of patients who did not improve on AS. Now with more patients using AS, there is about a 4-5% chance it will not help. If AS does not help, we recommend using Platelet Rich Plasma. I only have 4 patients to date out of hundreds who did not feel improvement with PRP drops.
Q. How long do Autologous Serum drops last? Depending on how often you use them, the effectiveness of AS is 6 months in the freezer. (See Reference below). We generally recommend a small bottle of AS be kept in the refrigerator for 1 week only after being defrosted.
2. Q. How long can they be frozen?
The concentration of a spectrum of cytokines involved in corneal epithelial wound healing and the epitheliothrophic effect of serum are not significantly changed after a prolonged storage of 6 months at -20 °C. So they can last for 6months if frozen.
3. What concentration of Autologous Serum should I use?
See above. We usually start with 20% as most studies use 20%. But we have found some patients feel symptom relief with 50% or higher. Though uncommon, if a patient does not feel eye pain/drynees relief after using AS for 2-3 months at 100%, we then try autologous Platelet Rich Plasma (PRP).
4. How often should I use Autologous Serum drops?
Each patient’s eye reacts differently to different treatments. Some patients feel relief with AS when used 2x per day. Some patients do well with 4x/ per day. Some do need to use the serum even every hour to get full relief. It is ok to start at 2x per day to see if this helps, if not, try to get in 4x/day as much as possible. If you work full time and cannot take a frozen AS or be sure the AS will be cold at work, use the AS more often on weekends. If still not better after 2 weeks, try going up even more if you can. Most patients feel full relief with Autologous Serum: it is just a matter of how often they need to use it initially and how quickly once can then back down on the drops.
5. How Long Will I Need to Use Autologous Serum?
Again each patient can respond differently. I have some patients who only need one 3 month course of AS and never need it again. Some can come off the drops and feel better for years after one course; some need their serum for life. We do not know why some patients get better forever with one course and others do not. We expect it has to do with immune status issues, baseline autoimmune disease risk, history of long term contact lens use, LASIK/PRK risk, history of Accutane, Chemo, Radiation, cancer, genetics, aging, hormones.
6. Is it ok to keep a defrosted bottle in the refrigerator for 7-10days?
The biggest risk of AS is corneal infection. I have never seen one but it has been reported. Keeping all bottles frozen until you plan to use it is key and then keeping the defrosted bottle in a cold refrigerator will ensure no bacteria grows in the non-preserved autologous serum. If you have any worsening pain, let us know right away: Ihave never had an eye infection on autologous serum even if used for 7-10 days as long as it is kept refrigerated (and others are kept frozen until ready to use).
.
More Questions and Answers About PRP (Platelet Rich Plasma):
1. How much blood do you need to withdraw?
We extract a small amount of blood (15-30mL) in most cases. Some patients traveling abroad request more PRP in which case we remove more blood over 2-3 days. The amount of blood we rithdraw is considered to be a relatively small amount of your total body’s blood supply. Depending on the weight and height of a person, the human body contains approximately 15 Gallons or 5L of blood. Thus30mL represents less than 1% of your total body’s blood supply.
Once a patients blood is extracted in a standard fashion, it is placed into a centrifuge. Only 1 person’s blood is placed into the centrifuge at all times. The centrifuge separates the parts of the blood into your Serum and PRP.
The entire process of preparing the PRP takes about 1 hour. If we make PRP on the same day as a visit, we allot 3 hours for the PRP to be ready given scheduling.
2. How Safe is PRP and how do you ensure the safety of PRP?
The safety of all our patients and employees is our #1 priority! We have been making PRP in our office under sterile conditions since 2016. We have never had a case of infection or any adverse side effect with PRP.
The following protocols and policies help to ensure the safety of PRP.
Sterile Needles, Single-Use Needles and Syringes are used: Only sterile and single-use surgical-grade needles and syringes are used. Once they are used on a person, they are immediately placed into a sharps bin for safe disposal.
Blood Collection: Only 1 persons blood is placed into the centrifuge at all times. This decreases any chance for any mix-up or cross contamination.
Hand Hygiene: Staff and patients always use the alcohol-based hand wash sanitizer that is provided in every room before handling blood products.
Sterile Drapes, Face mask, sterile gloves: Prior to making the PRP, a sterile gown, face mask, and sterile gloves are used to assure the sterility of the procedure. Our team is trained on the importance of following the sterile procedure protocol to ensure pathogens are not passed on.
Nothing is re-used: During the PRP making process, items that come in contact with your blood or any bodily fluid is immediately disposed of after use in an assigned compliant container. Nothing is reused if it comes in contact with your blood or any other bodily fluid when we make the drops.
3. Do any insurances cover PRP:
Unfortunately, Medicare does not presently offer any coverage for PRP, nor any other insurance that we know of. PRP does qualify for Flexible Medical Spending use: check with your employer to be sure.
4. Q. Is it a hard and fast rule to use PRP drops for 7 days, or can that be pushed to 8-10 days if there are still some remaining?
Dr. Cremers: Yes, it can be extended. The key risk, though very rare, of PRP and Autologous serum drops is the risk of infection. I have not seen anyone have an infection after PRP or Autologous serum drops made with Visionary Eye Doctors and we have used PRP drops for eye infections for patients given PRP's ability to heal. However, since your PRP and Autologous serum bottles have no preservative, these bottles cannot be left out on the counter. If a bottle start to turn murky, cloudy, or smell foul, do not use: throw it out. If you start to have any new yellow or green discharge, call us immediately. If you start to have eye pain while using PRP or Autologous serum drops, call us immediately.
5. More questions about PRP:
See blog post: https://www.blogger.com/blogger.g?tab=mj&blogID=1301797728403492391#allposts
Questions & Answers about Punctal Plugs:
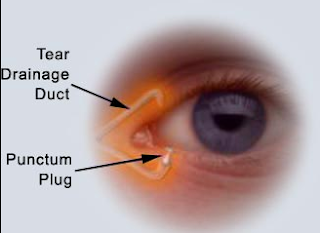
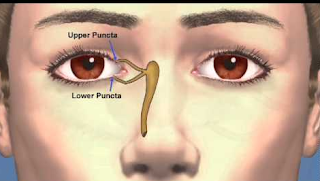
1. Q: What are punctal plugs?
A: Punctal plugs are a small medical device made from collagen or silicone which is inserted into the tear duct (puncta) of an eye to block the duct to prevents the drainage of tears from the eye to the nose. They are used to treat dry eye.They also may be called a tear duct plug or lacrimal plug.
2. Q: "I have heard of some people having more dryness since the puncta gets ‘stretched out’ and then drains too many tears."
A: Never heard of this or seen it published, though possible. So far no studies to prove this to date.
3. What are the complications of punctal plugs?
A: The vast majority of patient tolerate punctal plugs well.
If there are any side effects, which are rare, the plug can be easily removed in 99% of cases.
The most common side effect is excessive tearing: the plug can be removed in such cases.
Rarely will a patient note worsening of symptoms (because the eye is not able to flush out allergens or debris).
Treating blepharitis (inflammation of the lid margin) and keeping the eyelashes and lid margin clean, help prevent worsening symptoms after placement.
Rarely will a patient feel the plug due to the patient's anatomy that makes the plug rub against the conjunctiva: the plug can be removed in this case and tried in the upper puncta if placed in lower one or vice versa.
Infection around the plug is another risk but also very rare: I have seen only 2 in my career and they were placed by a different doctor.
I have never seen a plug get stuck in the canal and need surgical removal, but this has been reported--but very rare.
Contact Lens Question: More Questions: CL Question
1. Is it safer to have LASIK or wear contact lenses the rest of my life?
Great question. It depends on the status of your meibomian glands, your profession, and other risk factors. If a patient has severe meibomian gland atrophy, I would not recommend LASIK or PRK or any refractive surgery procedure except for cataract surgery or refractive lens exchange if patient cannot tolerate glasses (which is best option).
Many patients with mild and moderate Meibomian gland atrophy do not develop LASIK/PRK-related Dry eye but because I see the worst of the worst of these patients, I would only recommend LASIK/PRK in patient who fit the following criteria:
1. Never had Accutane
2. Grade 0-1 Meibomian (ie, normal meibomian glands)
3. Has no autoimmune disease
4. Has a topography that is completely normal and no signs of ectasia/keratoconus
5. Requires LASIK/PRK for work and is willing to accept risks of chronic dry eye, glare, halos, needing corneal transplant which is very rare.
2. How often should I use my contact lenses?
The less, the better. If you have stage 2 meibomian gland loss, I recommend less than 4 hrs of contact lens use. Using contact lenses more, will likely mean you will need to stop using them at an early age, but we have no studies to prove this or the time frame.
Patients with stage 3-4 gland loss: I recommend avoid contact lenses.
Patients with any keratitis for any reason: avoid contact lenses.
If you have any discomfort when inserting a contact lens, take it out immediately. Any persistent pain, discomfort, discharge, vision changes, redness requires immediate evaluations by an eye doctor ASAP: as in go to the Emergency room to be sure you do not have a corneal infection which can be blinding.
AUTOLOGOUS STEM CELLS:
Background:
Dry Eye Disease (DED) affects millions of patients globally.1, 2-13 DED is a common condition in which the normal tear film is inadequate to properly lubricate the eye’s cells and prevent pain sensation. For research purposes, DED is defined as a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film, and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles.1 For many patients, Dry Eye Disease can cause a severe, debilitating chronic pain syndrome, which has been shown to affect quality of life scores to the same effect of moderate/severe angina in adults.2
Researchers now know that the meibomian glands, which produce the precious oil in charge of preventing pain sensation in the eye, are a key component to the production of a normal tears. Additionally it is known that meibomian gland dysfunction (MGD) and Sjögren and non-Sjögren lacrimal disease are the leading causes of evaporative and aqueous-deficient DED, respectively. There are multiple risk factors (such as aging, computer use, Accutane (isotretinoin) use, contact lens use, autoimmune disease, radiation/chemotherapy) and causes of dry eye disease. However, the underlying issue is chronic inflammation that leads to a vicious cycle of tear hyperosmolarity, continuous inflammation, and scar tissue formation at the cellular and organ level of the meibomian glands, the lacrimal gland, and likely mucin cell layer.
All eye surgeons around the world see patients with dry eye complaints daily. The ubiquity of electronic screens is leading to an unprecedented rise in dry eye complaints in young adults and now children. There is a race against time to save the meibomian glands before they fully atrophy.
Currently, the treatments for dry eye do little to treat the underlying dysfunction of these meibomian glands. Most treatments, such as lid hygiene, artificial tears, increased Omega 3 intake, Xiidra®, Restasis®, punctal plugs, amniotic membrane, doxycycline pills, steroids (which increase risk for cataract and glaucoma), and autologous serum drops try to minimize inflammation, but there is no proof that these treatments rejuvenate these precious oil glands.
Meibomian gland probing and expression, LIPIFLOW, or Intense Pulse Light (IPL) therapy attempts to rejuvenate meibomian glands, and have been shown to help provide relief in many patients. However, these may not help some patients, and in other patients provides temporary relief of pain. These are not curative treatments.
Since my work at Harvard Medical School, I continue to see thousands of patients with Dry Eye Disease in private practice. I have had a special interest in DED ever since my research with Dr. Judah Folkman at Harvard Medical School on the angiogenesis basis of ocular rosacea and its effects on dry eyes and meibomian gland dysfunction. Patients from many parts of the world have travelled to the office to consult with me over the chronic pain they experience from dry eyes. This is a devastating condition in which young people are having to quit their jobs because they can no longer cope with the pain. Currently, we are about to submit a paper to the New England Journal of Medicine, noting the devastating consequences dry eye is having on young children aged 6-17. My interest is thus to help find a cure for dry eye disease. I am hopeful that stem cell injections may be that cure we are all looking for long term.
In an effort to find a cure for dry eyes, it became clear that a patient’s own stem cells is likely the key answer. Prior to the use of stem cells, though, I noted that a patient’s platelet rich plasma also contained many growth factors and some concentration of a patient’s own stem cells. Two of my patients with severe Sjogrens syndrome asked to try an injection of platelet rich plasma into their meibomian glands. Surprisingly the atrophied meibomian glands noted prior to the procedure on meibography, appeared to “grow back” clearly on the post-procedure meibography.
Given the nature of autoimmune diseases, it is not clear, though, how long this positive effect will last and whether stem cell injections into the meibomian glands present a possible cure for dry eyes or a better treatment option than what is currently available to patients.
Thus I have embarked on the study of autologous stem cell injections into the meibomian glands, lacrimal glands, and limbal stem cells of patients with a protocol created by the Cell Surgical Network®, California (CSN), which is a network of physicians in the US who use the same sterile closed surgical procedure to process fat from a mini-liposuction procedure in order to isolate and implant a patient’s own source of regenerative cells on the same day.
The regenerative cells are found in this adipose-derived stem cells as stromal vascular fraction, (SVF) which contains a mononuclear cell line (predominantly 2 types of autologous mesenchymal stem cells), macrophage cells, endothelial cells, immune regulatory cells, and important growth factors that facilitate the stem cell processes and promote their activity. This technology will allow us to isolate high numbers of viable cells that we can deploy during the same surgical setting, and inject the fresh stem cells into the meibomian glands, lacrimal glands, and/or limbal stem cell. The Cell Surgical Network® (CSN) is the group we will be partnering with and purchasing the equipment from. CSN is the world’s largest regenerative medicine clinical research organization and helps with the collection of data from affiliate centers all over the world.
My hypothesis is that stem cell injections will regenerate the patient’s cells involved in producing a stable, complete tear, which have been damaged by medications, autoimmune disease, aging, chemotherapy/radiation, chronic inflammation, excessive screen time, or other causes. This procedure is completely experimental, as there have been no studies to prove its effectiveness to date.
My protocol is as follows:
Consultation with Dr. Cremers to identify the key component of dry eye: meibomian gland dysfunction and/or aqueous tear deficiency
Schirmers testing, tear break up times, Lissamine green staining, OSDI questionnaires, and a lifestyle questionnaire asking about electronic screen use is administered before the procedure.
Type A patients: A patient with a normal schirmer’s test and normal blood work testing (ie, SJO, ANA, RF), would be considered a “non-autoimmune disease risk” patient. These patients likely need stem cell injection in only the meibomian glands and would be followed as such.
Type B patients: Patients with an abnormal schirmer’s test and/or abnormal blood work testing (ie, SJO, ANA, RF), would be considered an “autoimmune disease risk” patient and would possibly benefit from autologous stem cell injections into the meibomian glands and lacrimal glands.
Type C patients: Patients who had previous accutane use would be treated as type A patients if their Schirmer’s test is normal. If these patients have an abnormal Schirmer’s test and/or have any autoimmune markers that are positive, they will be treated as type B patients.
Type D patients: Patients who have chronic pain after LASIK or PRK would likely benefit from autologous stem cell injections around the corneal limbus in attempts to regenerate the corneal stem cells. These patients may also benefit from meibomian gland injections and thus both would be performed.
Once the type of patient is identified, the protocol is as follows.
Formal consultation and patient classification for injection identified
Consent form is reviewed with patient
CSN protocol is followed for procurement of stem cells in the form of stromal vascular fraction per their protocol: see attached articles regarding the details of the protocol which is derived from adipose tissue and their research results. A CSN surgeon will train Dr. Cremers and a CSN representative will train our staff to be sure we use their same protocol.
Meibomian gland probing and expression is performed according to Dr. Sandra Cremers’ current protocol of both eyes.
The adipose-derived stem cells in the form of stromal vascular fraction will then be injected into the designated area under a sterile technique of one eye (as the case eye) and the other eye (treated as a control eye) will not have any stem cell injections, similar to the current PRP injection protocol Dr. Cremers is currently using.
Patient is then followed at Week 4, 8, and 12 for standard testing including meibography of all four lids, Schirmer’s testing, tear break up time, lisamine staining. Ideally funding could be obtained to assess patients Tear Osmolarity and MMP 9 at the pre-procedure and post-procedure visits.
In type B patients, discussion on the use of ATCHAR will be discussed: see http://eyedoc2020.blogspot.com/2018/01/new-treatment-called-acthar-may-help.html
More Information:
http://eyedoc2020.blogspot.com/2017/05/stem-cell-injection-into-meibomian_5.html
Questions & Answers:
How many patients have been treated with Stem Cell Insertion into the Meibomian Glands?
There were 3 total.
How did they lose their meibomian glands or were their dry eyes because of something different?
1 patient had neuropathy from previous trauma.
1 had diagnosed Sjögren's syndrome.
1 had Accutane but also had positive early Sjögren's markers.
Still I do not totally understand how the pain has returned after half a year. Did the recovered glands (or some of them) disappear again and is it possible to repeat the stem cell treatment in such a case?
I believe the pain and dry eye symptoms improved because the Meibomian gland cells worked better to produce better quality meibum/oil. The underyling autoimmne destruction of Meibomian gland cells and lacrimal gland cells likely caused the pain/dry eye symptoms to return in the patients with underlying autoimmune issues. The patient with the neuropathy also improved but not as much as the other 2 patients: likely the stem cells worked to improve local nerve growth factor concentrations but was not a full cure to repair damaged/malfunctioning nerve cells.
Has someone done this for a second time yet?
One of the patients is returning for a second round.
What exactly are platelet-rich injections?
Autologous platelets are inserted into each Meibomian gland after probing and expression.
More information is noted here:
http://eyedoc2020.blogspot.com/2017/09/injection-of-platelet-rich-plasma-into.html
https://ascrs.confex.com/ascrs/18am/meetingapp.cgi/Paper/48067
CORD BLOOD SERUM:
Our first patient to have Cord Blood Serum for corneal neuropathy and trigeminal neuralgia reported a significant improvement in pain scores from 9/10 pain to 2/10 pain in the one eye the patient is using the CBS.
We are very excited about her initial pain scores. This patient will be returning for formal testing of Tear Break Up Times (TBUT), meibography, Schirmers's test and microscopic exams as well.
1. What is Cord Blood Serum?
Cord Blood Serum or Umbilical cord blood serum, has been used to heal corneal ulcer, erosions, neuropathy, severe dry eye, persistent epithelial defects, neurotrophic keratopathy, recurrent corneal erosions, ocular chemical burn, and corneal refractive surgery (Ref 2-8 below). Studies have shown that Umbilical Cord Blood (UCB) contains a higher level of growth factors, nerve growth factor, and other neurotrophic factors than compared to Autologous Serum.
We are now offering this to patients. We have an IRB approval to study the effects of cord blood in comparison to using Autologous, Adipose Derived, Stem Cells (AADSC) inserted into the meibomian glands. Our hope is to have patients use cord blood drops in one eye and have AADSC insertion into the meibomian glands of the other eye and compare the results over 1, 3, 6mo, 1yr, 3yr.
For now, we are providing Cord Blood drops to patients who have not found relief with all other options.
The next question is: since Cord Blood cells can become Nerve Growth Factor, will using Cord Blood drops work better or as well as NGF, especially in patients who have corneal neuropathy?
Studies below have shown Cord Blood is safe and effective. Still it is experimental and not FDA approved.
There is a recent paper noted below ** that indicated Cord Blood Serum may help patients with Glaucoma. The theory is that CBS contains a combination of GFs, which potentially exert a neuroprotective action to help prevent optic nerve damage and blindness. CBS, the authors note, is a natural source to potentially protect against neurodegenerative ocular disorders. They report that 2 patients showed improvement of their Mean Deviation and Pattern Standard Deviation on visual fields. They note that this incidentally observed amelioration in these two patients deserves further investigation in this respect.
They report only 2 cases, and the study has many confounding factors: for instance, maybe the CBS improved the patients' tear film so they did better on the repeat Visual Field test because of improvements in the tear film alone and not because of an actual improvement in optic nerve function. But the report is interesting none the less.
No side effects have been published with using UCB in the eye, but the same is true for Autologous Serum: UCB must be kept frozen and refrigerated as follows:
1. Unopened bottles MUST be stored in a freezer at -20℃. Can last for 3 to 6 months.
2. Opened bottles MUST be kept in a refrigerator at 4℃ for 7 days, and then Thrown OUT.
3. Drops cannot be left out.
4. UCS eye drops are usually instilled 4 to 6 times per day as required in addition to non-preserved artificial tears, Xiidra or Restasis if using, and an antibiotic drop (ie, Moxifloxacin 2x/day).
Here is the protocol we will be following:
Consent Form From donors: laboratory examination should be performed at 8 and 38 gestational weeks to test for human immunodeficiency and hepatitis B and C viruses.
After fetal delivery: about 60 to 80 ml of umbilical cord blood is sampled from the umbilical cord vein. The blood is kept for 2 hours at room temperature. After 15 minutes of centrifugation at 3,000 ×g, the serum is carefully isolated under sterile conditions. The serum is then diluted to a 20% concentration with balanced salt solution. The aliquots of diluted serum are placed into sterile 5-ml bottles with ultraviolet light protection.
Opened bottles are kept in a refrigerator at 4℃ for 7 days, and unopened bottles are stored in a freezer at -20℃ for 3 to 6 months. UCS eye drops are usually instilled 4 to 6 times per day as required in addition to artificial tears and antibiotics.
See: http://eyedoc2020.blogspot.com/2018/08/cord-blood-drops-for-dry-eye-disease.html?q=cord+blood+serum
DRY MOUTH: TOP 14 Causes of DRY MOUTH
1. Dehydration
2. Being a Mouth Breather, especially at night time: if you wake up with a dry mouth, this is most commonly the reason.
3. Medications. Many medications, including many over-the-counter drugs, produce dry mouth as a side effect. The biggest culprits are anti-depressants & medications to treat high blood pressure and anxiety, as well as some antihistamines, decongestants, muscle relaxants and pain medications.
3. Aging. Many older people complain of dry mouth as they age. Contributing factors include the use of certain medications, changes in the body's ability to process medication, inadequate nutrition, and having long-term health problems.
4. Allergies: the sensation of dry mouth is likely due to the resulting inflammation from the allergies.
5. Tobacco and alcohol use. Drinking alcohol and smoking or chewing tobacco can increase dry mouth symptoms. Hopefully, no one out there smokes anymore.
6. Diabetes: since Diabetes is an epidemic, get checked for diabetes with a HgA1C. Polydipsia, or always being thirsty is a key symptom.
7. Autoimmune disease, like Sjogren's syndrome: the SJO test can sometimes help determine if you are on the spectrum of Sjogren's syndrome and confirm advanced disease.
8. Cancer therapy. Chemotherapy drugs can change the nature of saliva and the amount produced. This may be temporary, with normal salivary flow returning after treatment is completed. Radiation treatments to your head and neck can damage salivary glands, causing a marked decrease in saliva production. This may be temporary or permanent, depending on the radiation dose and area treated.
9. Yeast infection in mouth: ie Thrush.
10. Nerve damage. An injury or surgery that causes nerve damage to your head and neck area can result in dry mouth.
11. Stroke: if previous history of Stroke, dry mouth can result.
12. Alzheimer's disease
13. HIV/AIDS
14. Recreational drug use. Marijuana & Methamphetamine use can cause severe dry mouth and damage to teeth, a condition also known as "meth mouth."
*If you have any other questions that are not included on this sheet, please email them directly to jramirez@voeye.com
_____________________________________________________________________________________
Created and edited by: Dr. Sandra L. Cremers, Loi Vo, and Allie Blankenship
Updated January 2019
References:
1. https://ejhp.bmj.com/content/24/Suppl_1/A205.1
PP-008 Stability and sterility of autologous serum eye-drops after long term storage
D Wandel1,
L Bernasconi2,
R Egger1
Abstract
Background Autologous serum can be compounded into eye drops that are used to reduce symptoms of severe dry eye syndrome. In the case of appropriate stability and sterility, frequency of blood drawings from patients might be reduced and clinical logistics simplified.
Purpose To assess the sterility and stability of serum under different storage conditions and prolonged storage time up to 6 months.
Material and methods After obtaining whole blood and preparing unit dose autologous serum eye drops 100% and 50%, samples were stored at 4°C and −20°C for up to 6 months. Concentrations of albumin, immunoglobulin G and C4 (C4c) were used as surrogate stability biomarkers and measured on storage days 1, 8, 15, 30, 60, 90 and 180. Sterility according to European Pharmacopoeia (2.6.1) was evaluated on storage days 1, 15, 30, 60, 90 and 180.
Results The concentrations of albumin and immunoglobulin G remained stable under both temperature conditions over the entire period of 6 months. The C4c concentration increased by about 30% at storage temperature of 4°C. This was not the case for samples stored at −20°C. No difference in C4c concentrations was seen between undiluted and diluted serum. Sterility was maintained in the 4°C and −20°C samples throughout the period tested.
Conclusion The present results show that serum parameters albumin, immunoglobulin G and C4c are stable at −20°C for 6 months. As C4c is a breakdown product of C4b, the increase in C4c at 4°C may be indicative for some instability of C4b. However, this increase is considered mild and values remained within the normal range, and hence this change may have no clinical significance. At both temperatures tested, sterility of serum eye drops was not impacted, including the longest storage duration tested. In summary, the results support using aseptic preparation techniques and storage temperature at −20°C. A 6 month supply of autologous serum eye drops can be offered to patients, allowing better access to this therapy through a less frequent blood donation schedule.
No conflict of interest
Here is a good interview about Meibomian Gland Probing with Dr. Maskin in Eyeworld October 2017
Meibomian gland probing: The who, what, where, when, and why by Liz Hillman EyeWorld Staff Writer Meibomian gland intraductal probing of the upper lid to relieve fixed and non-fixed obstructions Source: Steven Maskin, MD Watch Dr. Maskin perform meibomian gland probing on several patients. Watch a patient’s testimonial of this procedure. See Dr. Maskin release trapped meibum with meibomian gland probing. Complete distal obstruction (left), as indicated by the orange band around the meibomian gland illustration, and complete proximal obstruction (right) show two different types of gland atrophy that could result from an obstruction and subsequent meibum buildup and pressure. Source: British Journal of Ophthalmology/Steven Maskin, MD The scoop on the technique that aims to relieve obstructive meibomian glands Steven Maskin, MD, Dry Eye and Cornea Treatment Center, Tampa, Florida, first introduced the idea of inserting a wire probe into meibomian glands to relieve obstructions that could be causing discomfort and dry eye in 2010.1 Since then research has shown it to be, what he called, a “paradigm shift” in successful treatment of obstructive meibomian gland disease.2–4 Dr. Maskin gave EyeWorld an in-depth look at his tips and tricks on meibomian gland probing (MGP). EyeWorld: What is MGP? Dr. Maskin: Meibomian gland probing is the introduction of a wire instrument to the gland orifice with insertion through the orifice and into the ductal outflow tract. EyeWorld: What’s the purpose of probing? Dr. Maskin: Probing establishes and confirms with positive physical proof a patent outflow channel including duct and orifice. Probing, by relief of intraductal obstruction, is therefore able to equilibrate intraductal pressures within the duct and promote removal of sequestered and other retained intraductal contents. At times, the introduction of intraductal lavage or microtube injection of pharmaceutical will act to remove material that was not released with probing and subsequent expression alone. In summary, initial and maintenance probing: (1) relieves obstruction, (2) maintains patency of outflow channel, and (3) is associated with growth of meibomian gland tissue. EyeWorld: What are the indications? Dr. Maskin: Probing has become a first-line treatment for MGD in my practice to eliminate intraductal resistance to meibum flow from all types of obstruction. This includes fixed, unyielding obstruction such as periductal fibroses as well as non-fixed obstruction such as thickened meibum and hyperkeratinization. I also use it for gland maintenance to help prevent initial or progressive atrophy similar to a dental analogy of periodic prophylactic tooth scaling and cleaning. Now that we have seen and published on growth of gland tissue after probing, we are also exploring the use of probing with adjunctive injection therapies to further stimulate gland growth and restoration of a full, functional, healthy, and resilient meibomian gland lid population.5 I use probing on patients with lid tenderness over the meibomian glands (indicating elevated intraductal pressure). Probing dramatically and immediately relieves lid tenderness from elevated intraductal pressures. I use probing to restore functionality to non-meibum expressing glands, as well as to relieve symptoms of lipid tear deficiency. I also use probing to stimulate growth of gland tissue from glands with dropout or atrophy on meibography. EyeWorld: Can you describe the probes used for MGP? Dr. Maskin: The stainless steel probes are 76 µm in diameter with lengths of 1, 2, 4, and 6 mm. The probes are non-sharp to minimize alteration of tissue and allow the physician to better feel the tissue and resistance during the probing procedure rather than sharp blades that would slice their way through the tissue without yielding diagnostic information about the type and extent of resistance as well as likely cut through the duct wall, creating a false passage. Stainless steel is important to give the probe a stiffness to allow safe and quick penetration through the orifice and into the duct. EyeWorld: How do you anesthetize a patient for this procedure? Dr. Maskin: I use my patented jojoba-based anesthetic ointment (JAO) containing 8% lidocaine available from O’Brien Pharmacy (Mission, Kansas). After placing one drop of topical anesthetic into the inferior fornix, I place a bandage contact lens on the eye and a generous amount of JAO on the lower lid margins. The eye is closed for 10–15 minutes during which time both upper and lower lid margins are anesthetized. The eye is opened and a second drop of topical anesthetic is placed in the inferior fornix. If the patient’s lids are still sensitive after probing has begun, a second round of JOA applied to the lid margin is typically successful in making the procedure well tolerated. After probing is completed, the contact lens is removed and the ocular surface is copiously irrigated with sterile preservative-free saline. Then a cotton-tipped applicator is used to remove any residual JAO from eyelashes. EyeWorld: Are there different approaches to anesthesia? Dr. Maskin: An alternative approach uses topical proparacaine on the ocular surface followed by a corneal protective shell and a cotton pledget soaked in 4% lidocaine placed into the fornix for 5 minutes. Then 1% lidocaine with epinephrine is injected using a transconjunctival approach into the fornix centrally, medially, and laterally with supplemental subcutaneous injection near the eyelid margin.4 EyeWorld: How is the patient positioned during the procedure? Dr. Maskin: While anesthetic is applied in a reclined position for MGP, I position the patient at the slit lamp for virtually all my probing. An assistant is there to support the back of the head, if necessary. Other physicians may prefer reclining a patient on a surgical chair and using an operating microscope. EyeWorld: MGP can involve different probe lengths; how is probe length selected? Dr. Maskin: I always begin with the 1-mm probe. The 1-mm probe is the shortest and stiffest and therefore most likely to penetrate through orifice or distal duct fibrosis or other unyielding fixed obstruction. Longer probes are used if there is persistent lid tenderness over a gland suggesting deeper obstruction with elevated intraductal pressure. Longer probes can also be used to reach into a developing hordeolum to promote drainage. When using longer probes, always use progressively longer increments. After the 1-mm, use 2-mm, and then 4-mm probes, if necessary. EyeWorld: How do you decide which glands are probed? Dr. Maskin: I probe all orifices. This is important as I have seen glands with minimal associated acini restored to functionality after probing and start expressing meibum. Furthermore, now that we know there can be post-probing growth of meibomian gland tissue from previously atrophic glands, it is important to stimulate growth associated with all orifices and/or glands.5 EyeWorld: What techniques do you use to identify the gland orifice and insert the probe? Dr. Maskin: It is usually not difficult to identify orifices. Some physicians use red-free light to assist. Transillumination or meibography can reveal location of glands as well. Rest the tip of the 1-mm probe on the orifice. Using a dart-throwing motion, try to insert the probe into and through the orifice. This is done by holding the probe handle as you would hold a dart and using a short jab motion of 1–2 mm to penetrate through the orifice into the duct. The probe will enter the duct naturally and the duct itself will guide the probe, similar to your arm entering the sleeve of a shirt. If you meet resistance, try a different entry angle for the dart-throw motion. The orifices and distal ducts may be dragged posteriorly or fibrosed in a way that requires an altered entry angle. EyeWorld: Could the probe create a false passage? Dr. Maskin: Probing does not create a false passage. When you penetrate the orifice and enter the gland, the effect is tantamount to passing your arm into your shirtsleeve. The probe simply follows the duct in the same fashion. EyeWorld: What is the importance of probes being “non-sharp”? Dr. Maskin: Probing is both a first-line treatment as well as a diagnostic test looking at the frequency and type of gland resistance, which may correlate with severity of symptoms. It is important when probing to do so effectively with minimal unnecessary disturbance of gland tissue. It should be noted that a post-probing confocal microscopy study has shown no degenerative changes in morphology of meibomian gland acinar units or meibomian gland scars.3 EyeWorld: What are the procedural findings of probing? Dr. Maskin: When the probe is inserted through the orifice and into the central duct, you quickly encounter orifice and/or ductal resistance. This resistance may be relieved by advancing with the probe, generating an audible and tactile sensation of a “pop” or multiple pops causing an audible and tactile “gritty” sensation. The also patient hears and feels the pops and gritty sensation and can appreciate the instant relief of elevated intraductal pressure as the obstruction is relieved, intraductal pressures equilibrate, and meibum flow is restored with relief of tenderness. Lid tenderness is dramatically and immediately relieved. Persistent lid tenderness suggests deeper obstruction requiring probing with a 2-mm or 4-mm probe. EyeWorld: Is trapped meibum released? Dr. Maskin: As the intraductal obstruction is relieved, you frequently see sequestered meibum release along the wire probe to exit through the now patent outflow channel and through the orifice. EyeWorld: What about hemorrhages? Dr. Maskin: Dot hemorrhages frequently appear at the orifice. These hemorrhages are self-limited and do not need pressure or any treatment. EyeWorld: Is MGD something a tech could do? Dr. Maskin: I can see the day when a trained physician assistant could do it. EyeWorld: Is there any way to inject medication into glands after probing? Dr. Maskin: Yes. With 110 and 152 µm tubes, we can deliver medication directly inside the gland, such as dexamethasone or small particle suspensions. Injections directly into the gland enable targeted treatment of gland dysfunction as well as removal of stagnant secretions with an irrigation or lavage approach. Early studies suggest we have found an adjunct microtube injection treatment to prolong onset of recurrent intraductal obstruction and reduce orifice hemorrhage upon retreatment probing. This would be meibomian gland orifice and duct reconstruction. We are also exploring the use of probing with adjunctive injection therapies to further stimulate gland growth and restore a full, functional, healthy, and resilient meibomian gland lid population. EyeWorld: What should you be looking for on follow-up visits? Dr. Maskin: It is important to remember that MGD with progressive gland atrophy can and will occur at a subclinical level without symptoms. Patients with symptoms relieved after probing who have become asymptomatic need to be monitored on every visit to detect early reobstruction with progression of disease even if the patient is symptom-free. This can include checking for lid tenderness and expressible glands on every exam plus meibography every few months. Symptom relief from MGP should last about 1 year. If symptoms reappear earlier or if there is a decrease in the number of expressible glands or increase in lid tenderness, there is an unrecognized or inadequately treated local, regional, or systemic comorbid disease. Probing provides positive physical proof of patency, but once achieved the patent outflow channel must be defended against all comorbid sources of inflammation that would reobstruct the outflow tract. References 1. Maskin SL. Intraductal meibomian gland probing relieves symptoms of obstructive meibomian gland dysfunction. Cornea. 2010;29:1145–52. 2. Maskin SL. Intraductal meibomian gland probing: A paradigm shift for the successful treatment of obstructive meibomian gland dysfunction. In: Kazuo Tsubota, ed. Diagnosis and Treatment of Meibomian Gland Dysfunction. Tokyo, Japan: Kanehara;2016:149–167. 3. Dongju Q, et al. Clinical research on intraductal meibomian gland probing in the treatment of patients with meibomian gland dysfunction. Chin J Optom Ophthalmol. 2014;16:615–21. 4. Syed ZA, et al. Dynamic intraductal meibomian probing: A modified approach to the treatment of obstructive meibomian gland dysfunction. Ophthal Plast Reconstr Surg. 2017;33:307–309. 5. Maskin SL, et al. Growth of meibomian gland tissue after intraductal meibomian gland probing in patients with obstructive meibomian gland dysfunction. British J Ophthalmol. 2017 June 7. Epub ahead of print. Editors’ note: Dr. Maskin owns patents on devices and methods of intraductal meibomian gland diagnosis, treatments, and topical therapies. He has financial interests with Rhein Medical (St. Petersburg, Florida).
https://www.eyeworld.org/meibomian-gland-probing-who-what-where-when-and-why
Source: https://www.eyeworld.org/
More Warm Compresses & Lid Hygiene Questions: the full post is here:
http://eyedoc2020.blogspot.com/2017/02/how-best-to-clean-my-eyelids-controversy.html?q=korb+towel
http://eyedoc2020.blogspot.com/2019/06/what-is-best-way-to-apply-warm.html?q=warm+compresses
Hopefully, more studies like the ones below will begin to shed light on the following questions everyone has:
1. How hot should the compress be?
2. For how long should I put the compress on?
3. How exactly should I do the warm compresses?
4. How many times a day should I apply warm compresses?
5. Should I massage my eyelid margin?
6. How should I massage my eyelid margin?
7. Should I self-express my glands?
8. What drops should I use?
9. Is it ok to wear makeup?
10. Should I throw out my makeup?
11. How best should I dilute the Tea Tree Oil?
12. Is Avenova equivalent truly to Tea Tree Oil in getting rid of Demodex?

But there is some data to answer some of these questions:
1. How hot should the compress be?
Dr. Korb and Dr. Blackie, who are excellent optometrists, have done the most research on this question that I could find thus far:
Reported melting temperatures of normal meibomian secretions vary significantly with the majority of reports ranging from 32 to 40°C; severely obstructed meibomian glands have considerably higher melting points. Only using mildly warm water may not be adequate to relieve the meibomian gland obstruction. Therefore, each degree of temperature increase over 40°C could be critical in melting severely obstructed material. However, increasing temperature without safety controls raises the issue of potential thermal damage to the cornea [though I have never seen this or read a case report of burning the cornea as one would usually have so much pain from burning the skin that it would not be possible to burn the cornea with just a hot compress]. Based on the most conservative safety thresholds in the literature, temperatures below 40°C will not result in thermal injury to the cornea or crystalline lens.(Reference 1 below)
They created the LIPIFLOW machine which provides steady state temperature of 42.5°C for 12 minutes at the eyelid margin.
For daily cleaning, this means the water should be very warm but not hot enough to cause pain or burn the skin.
2. For how long should I put the compress on?
Dr. Korb says 15minutes is the best. But no one I know really has 15 minutes 2-3 times per day to do there warm compresses. Thus it may be better to do warm compresses more often (but not within 2 hours of each session--see below) 3 times a day instead of 2 times a day for as long as you can.
3. How exactly should I do the warm compresses?
The only good study I could find to say it was superior is called the Bundle Method.
Again, the bundle methods sounds lovely, but most patients I know do not have time to do this. Thus any type of dry or wet heat helps. How much it will help for you depends on many factors: how many glands you have, is there any scaring in the glands, your age, your hormone status, what other meds are you on.
4. How many times a day should I apply warm compresses?
Likely the best is at least 2-3 times per day.
What we do know is from a study by Dr. Korb & Dr. Blackie: the below tells us, you need to apply some pressure (not too hard) on the eyelids for about 8-20 seconds

"The results show that a single central meibomian gland can be drained of its liquid secretion in 8-20 seconds upon application of a constant force of 1 g/mm2. After a central optimally secreting gland has been drained of its liquid secretion, it takes a mean time of 2.17 ± 0.49 hours to again secrete liquid during waking hours, using the same amount of force to express the new liquid secretion. At that serial expression when liquid secretion is first observed, it then takes approximately half of the time required to drain the gland originally to redrain the gland, indicating a partial recovery. Furthermore, the minimal amount of liquid secretion obtained upon diagnostic reexpression after drainage suggests that a meibomian gland in this condition may contain inadequate liquid secretion to be available with habitual blinking, which applies a force less than 1 g/mm2." Reference 3,4 below.
5. Should I massage my eyelid margin?
Yes. Studies show massaging pumps out the oil, especially if the oil has been melted with warm compresses beforehand.
6. How should I massage my eyelid margin? And can I massage my eyelids too much?
This is a controversial one. I recommend massaging for 20 seconds with warm water applied to eyelids at same time (mostly to save time), or with a warm compress as noted below. The key thing to remember is that the warmer the better but do not burn your skin. I have not heard of massaging your eyelid too much if there are no skin issues.

Both these options are good. I find the above one to be faster. If someone has a tremor or very long fingernails, I would avoid this bottom one to avoid a corneal abrasion.

7. Should I self-express my glands?
It depends on what we mean by "self-express." Some patients I know pinch their eyelid margin trying to push out the oil for relief. I could not find any studies to show this is dangerous, but my main concern would be a potential corneal abrasion from scratching the eye. Using an instrument to self express again would be a concern for potentially scratching the cornea. As long as this self expression is not done too aggressively, it makes does not seem to be dangerous. But again we do not have good studies to show it is dangerous that I could find.
8. What drops should I use?
There are many that can be used. The best is a non-preserved tear. A 'no-drug company money" study showed that Retaine is the best. I have a post on this which I will link up shortly.
9. Is it ok to wear makeup?
Likely yes as long as you are taking off the make up completely. I could not find any study saying make up permanently clogs the glands if removed. Many of my severe dry eye patients, though, have stopped being able to use make up as they do feel it makes their eyes feel worse even if they remove it completely.
10. Should I throw out my makeup?
When I was a resident, we used to recommend patients throw out their make up if we saw "Blepharitis"--the catch all phrase for bacteria and now Demodex mites seen on the microscope. We now know that the bacteria & mites will come back even if you get new make up. Likely it makes sense to throw out the make up every year or 2 but I do not have studies to back this up.
11. How best should I dilute the Tea Tree Oil?
Different patients and their skin prefer different dilutions. 50% dilution with coconut oil, mineral oil, olive oil is likely best. I use pure tea tree oil "diluted" on a warm wet towel to clean my eyes. Likely it does not dilute very much as oil and water do not mix, but this works best for me.
12. Is Avenova equivalent truly to Tea Tree Oil in getting rid of Demodex?
The Avenova company says they are but there are no head to head studies. I do use both and find both to work. I prefer Tea Tree Oil when my eyes feel particularly crusty or uncomfortable as one can feel it working. The Avenova feels like water but that is a good thing especially if you have very sensitive skin. My kids prefer Avenova!
References:
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.